
Egg donation clinics provide coordinated services that facilitate donation of human oocytes for assisted reproduction. A clinic typically manages recruitment and screening of potential donors, medical procedures for oocyte retrieval, counselling for donors and intended parents, and administrative tasks such as legal documentation and recordkeeping. Navigating the combined legal, ethical, and financial dimensions involves consideration of national and local regulations, professional medical standards, informed consent processes, and transparent arrangements for compensation and fees. The clinic environment often brings together medical teams, legal advisors, and psychosocial professionals to address the multiple interests involved in donation pathways.
Operationally, clinics may follow standardized clinical protocols for stimulation, monitoring, and retrieval while also implementing policies for donor eligibility, genetic and infectious disease screening, and counselling. Ethical issues commonly include considerations of donor autonomy, non-coercion, equitable access, and long-term records for offspring. Financial elements can include donor reimbursement, clinic fees, and third-party payer arrangements where permitted. Privacy and data protection are usually part of clinic policies, informing how donor identity, medical records, and future contact preferences are handled. These elements create an integrated framework that clinics manage alongside clinical care.

Medical screening and testing protocols typically combine several assessments to evaluate donor health and reproductive potential. These may include transvaginal ultrasound, hormone assays, infectious disease panels, and targeted genetic testing based on family history. Clinics often follow professional society guidance when selecting tests, and testing algorithms can vary by jurisdiction or clinic policy. Timing and sequencing of tests are usually structured to align with stimulation cycles, with results informing eligibility and risk counselling. Donors may be asked to provide comprehensive medical histories and to undergo repeated or follow‑up testing when indicated.
Informed consent and legal agreements often address the scope of donation, transfer of parental rights, and expectations about anonymity or contact. Consent documents may describe medical procedures, potential risks, and short‑term follow‑up care, while separate contracts can clarify financial arrangements and release of claims related to parental status. Clinics commonly recommend legal counselling to clarify rights and obligations, and some jurisdictions require specific statutory forms. Record retention policies for consent and identifying information may be defined by law or professional guidelines, and these records can affect future choices about contact and medical disclosure.
Compensation and fee structure models can vary across clinics and legal frameworks. Reimbursement models often separate direct donor-related expenses (travel, lost wages, medical costs) from payment for services rendered to intended parents, and some systems permit modest compensation while others restrict or prohibit payments beyond expense reimbursement. Clinics frequently provide itemized estimates for procedures, medications, and laboratory work, and may operate on a fee-for-service or bundled-fee basis. Financial transparency is commonly advised so donors and recipients understand which costs are covered and which are the responsibility of the parties involved.
Privacy and recordkeeping practices typically govern how donor medical data, identifying information, and offspring-related records are stored and accessed. Clinics may use secure electronic medical records, implement access controls, and outline policies for sharing information with recipients and authorized third parties. Options for anonymity versus identity disclosure can differ by jurisdiction and by donor preference when permitted. Some clinics also maintain long-term records that support future medical updates for offspring and enable contact arrangements established at the time of donation.
In summary, clinics that arrange egg donation integrate clinical protocols, legal documentation, ethical safeguards, and financial arrangements into a coordinated process. Each component may be influenced by local law, professional guidelines, and institutional policies, and stakeholders often consult multiple specialists to address complex issues. Further sections examine practical components in more detail, including medical screening, legal frameworks, financial arrangements, and privacy practices.
Medical and donor screening procedures are foundational to clinic operations and typically follow multi-step protocols. Initial screening often includes a detailed medical and reproductive history, physical examination, and baseline laboratory testing. Subsequent steps may include ovarian reserve assessment such as antral follicle count or anti‑Müllerian hormone measurement, hormonal monitoring during a stimulation cycle, and pre-procedure imaging. Infectious-disease testing and pharmacologic safety assessments are commonly included to reduce clinical risk to donors and recipients. Clinics may adapt specific testing panels based on professional guidance and evolving evidence.
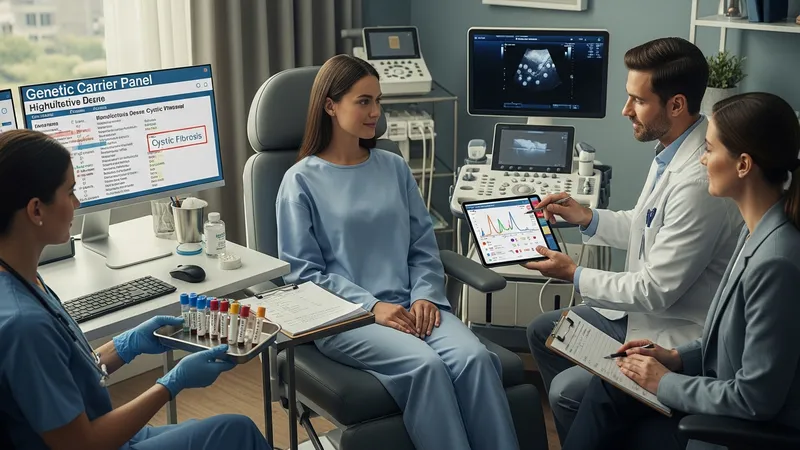
Genetic screening is frequently incorporated into donor assessment when indicated by family history or population-based risk patterns. Panels may range from carrier screening for specific recessive conditions to broader panels that evaluate multiple genes; selection of tests often considers clinical relevance and local practice. Genetic counselling is commonly offered to explain potential findings, implications for offspring, and options for recipients. Results can influence donor eligibility and decision-making, and clinics may set thresholds for disqualification based on identified risks.
Monitoring protocols during ovarian stimulation typically involve serial ultrasound and hormone measurements to guide medication dosing and timing of retrieval. These measures may help estimate follicular response and mitigate complications such as ovarian hyperstimulation syndrome, which clinics monitor using accepted clinical criteria. Post-procedure follow-up commonly includes short-term assessment for complications and recommendations for recovery. Clinics often document adverse events and may use collected data to refine protocols and safety measures over time.
Practical considerations for donors often include clarity about expected visits, potential side effects, and follow-up obligations. Clinics may discuss contraception recommendations after retrieval, options for future fertility, and availability of counselling resources. Donors may be advised that screening and procedures can reveal incidental findings requiring further evaluation, and clinics commonly have pathways for referral and documentation. These considerations inform informed consent and help align expectations for donors and recipients.
Legal and ethical frameworks shape the contractual and consent processes used by clinics and can vary by jurisdiction. Legal agreements commonly address parental rights transfer, donor releases, and arrangements concerning any future contact or disclosure. Some jurisdictions have statute-based provisions that define parentage and required consent forms, while others rely on case law and contractual practice. Ethical frameworks used by clinics often reflect professional guidance emphasizing voluntary consent, protection against coercion, non-exploitative practices, and attention to donor welfare.

Informed consent is a central ethical and legal concept; comprehensive consent processes typically cover procedure details, risks, potential outcomes, testing, and data use. Clinics often provide written materials and opportunities for verbal discussion, and some require a waiting period to ensure decisions are voluntary and informed. Ethical review mechanisms—such as institutional oversight or independent ethical consultation—may be used for complex cases or novel protocols, helping clinics navigate competing interests between donors and recipients.
Considerations about anonymity and future contact are ethically sensitive and legally variable. Some regulatory frameworks permit identifiable donor information to be released under defined circumstances or after specific timeframes; others protect donor anonymity. Clinics may offer choices about contact preferences where law allows, and policies typically document how records supporting contact are maintained. Ethical discussion around offspring access to donor information often weighs donor privacy against the potential health and identity interests of offspring.
Regulatory compliance and documentation practices can affect clinic operations and legal exposure. Recordkeeping requirements, reporting of adverse events, and adherence to clinical standards are commonly part of oversight by health authorities or professional bodies. Clinics may implement internal policies to align with regulatory expectations and to provide transparent documentation of consent, screening, and financial arrangements. These administrative practices support accountability and help clarify obligations for all parties involved.
Financial arrangements in egg donation processes typically separate clinical service fees from donor reimbursements and incidental expenses. Clinics may provide itemized fee schedules covering medications, monitoring, laboratory work, retrieval procedures, and storage where applicable. Donor-related reimbursements often address documented expenses such as travel and time off, and some systems incorporate compensation elements where legally permissible. Transparency about costs and the components included can help donors and recipients understand the financial dimensions of a given arrangement.

Contracts frequently articulate the scope of financial responsibilities and any conditions tied to reimbursement or compensation. Written agreements between donors and clinics often specify payment timing, coverage of medical care related to the procedure, and conditions under which payments may be adjusted. Intended parents and clinics may also agree on service terms that detail included services and potential additional costs such as storage or genetic testing. Clear contractual language is commonly recommended to reduce misunderstandings about financial obligations.
Payment logistics and third‑party payer involvement vary across contexts; some arrangements are entirely private while others may involve institutional facilitators or insurance coverage for particular services where allowed. Clinics may outline acceptable payment methods, invoicing practices, and refund policies for canceled cycles. When multiple parties are involved, allocation of financial responsibility and documentation of payments are often integral to administrative workflows and legal clarity.
Financial transparency is also an ethical consideration, as unclear or coercive financial practices can create undue influence. Clinics typically seek to balance fair reimbursement with avoidance of undue inducement, following applicable regulations and ethical guidelines. Donors may be encouraged to seek independent advice about contractual and financial terms, and clinics commonly document consent and financial agreements to support informed decision-making.
Privacy and record retention policies affect how clinics manage donor information, medical records, and requests for offspring access to data. Clinics often implement secure record systems and access controls to protect identifying information, while specifying conditions under which data may be shared with recipients, legal representatives, or authorized entities. Retention periods and policies for destruction or anonymization of records may be influenced by legal requirements and professional recommendations, and documentation typically reflects how future contact preferences are managed.
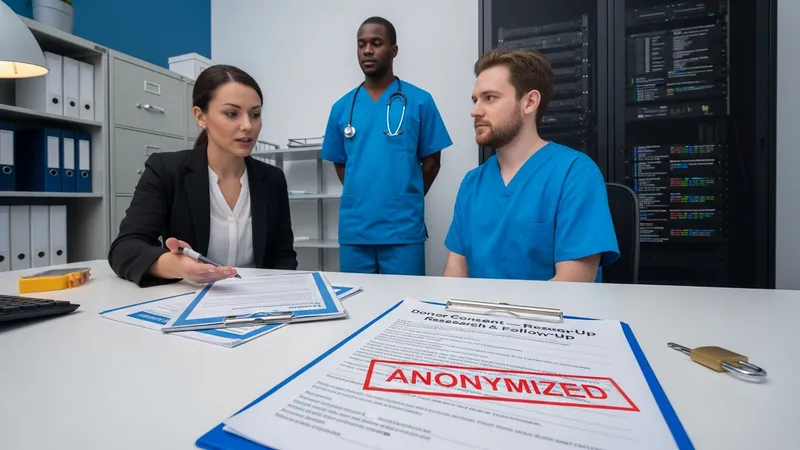
Data sharing practices for medical follow-up or research are commonly governed by consent agreements. Donors may be asked to authorize specific uses of anonymized or identifiable data for clinical follow-up or approved research, and clinics often outline the scope and limits of such use. Where research uses are contemplated, separate consent processes or ethics approvals may be employed. Clinics may also advise donors about potential implications of genetic or health-related findings for family members.
Clinical follow-up and reproductive healthcare practices for donors and recipients may include pre-procedure counselling, peri-procedural care, and recommendations for monitoring after retrieval. Clinics often coordinate with primary care or specialist providers when incidental issues arise, and may have agreements for referral to manage complications. Quality assurance practices such as tracking outcomes, adverse events, and protocol adherence can inform ongoing clinical improvements and compliance with professional standards.
Long-term considerations for offspring health and identity may influence clinic policies on recordkeeping and disclosure. Some clinics maintain options for limited or open records to support future access to medical or identifying information when appropriate and permitted by law. Decisions about record availability are often framed as part of the informed consent and contractual process, and clinics commonly document donor preferences and recipient expectations to guide future handling of inquiries or requests.